


Background: There is limited data to guide prescribing of all available anticoagulants in obese patients, in particular those weighing > 150kg or with a BMI > 40kg/m2. We aimed to examine anticoagulant prescribing patterns in obese patients in Australia and New Zealand including choice of agent and dosing, determine whether patients with obesity achieve appropriate direct oral anticoagulant (DOAC) levels and evaluate the efficacy and safety of anticoagulation in obese patients.
Methods: Patients with a BMI > 35kg/m2 or weight > 120kg receiving anticoagulant therapy are prospectively identified at 7 sites in Australia and New Zealand. Demographic data, indication for anticoagulation and choice of anticoagulant are collected at baseline. At follow-up visits, drug specific levels, dose adjustments and clinical progress (symptoms, imaging, recurrent thrombosis and adverse events) are recorded.
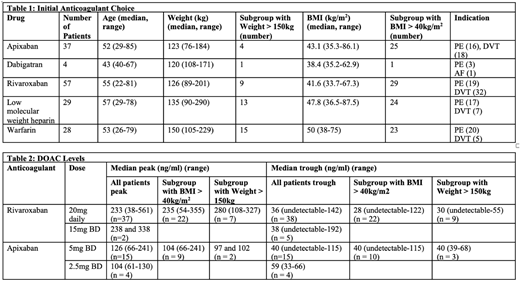
Results: 155 patients have been recruited across seven sites (recruitment ongoing). The median age of patients was 53 (range 22-85) and 49% of patients were male. 77 (50%) of patients were anticoagulated for pulmonary embolus (PE) while 40% were anticoagulated for deep vein thrombosis (DVT) without PE. Initial anticoagulant prescribed was apixaban in 37 patients, dabigatran in 4 patients, rivaroxaban in 57 patients, low molecular weight heparin (LMWH) in 29 patients and warfarin in 28 patients (Table 1). A subset of patients initially received LMWH for 5-14 days prior to transition to a DOAC (rivaroxaban in 7, dabigatran in 6). There was cross-over between agents during the study period.
Table 2 demonstrates median peak and trough DOAC levels. All peak apixaban levels and 25 of 37 (68%) peak rivaroxaban levels were within the therapeutic ranges published by the International Council for Standardization in Haematology (Gosselin, Thromb Haemost. 2018). Assessment of appropriate trough levels was limited by the limit of detection at different laboratories.
27 patients receiving enoxaparin had at least one peak Anti-Xa level (target peak 0.5-1.2U/ml). The median enoxaparin dose to achieve therapeutic peak Anti-Xa was 0.9mg/kg (range 0.52-1.3). 15 patients weighing > 150kg had a recorded peak Anti-Xa, 10 of these patients were prescribed a capped dose of 150mg BD (weight range 155-290kg) and nine had a therapeutic Anti-Xa and one had a supratherapeutic Anti-Xa measurement.
One patient had a PE on apixaban 5mg twice daily (in the setting of suspected non-compliance), one patient had a new confirmed PE after 4 days of non-compliance with rivaroxaban 20mg daily and another patient had a confirmed recurrence on therapeutic warfarin. 1 patient had a PE when warfarin was withheld for emergency surgery. An equivocal recurrence occurred on enoxaparin with a supratherapeutic Anti-Xa (1.76 U.ml) and 1 DVT occurred on dabigatran for a cardiac indication (no drug level available). One patient had recurrent superficial thrombophlebitis on rivaroxaban 20mg daily (peak 301ng/L and trough <30ng/L). There was one episode of life-threatening gastrointestinal bleeding on dabigatran.
Conclusion: There is limited data to guide prescribing of all anticoagulants in obese patients, in particular in patients weighing > 150kg or BMI > 40kg/m2. There is increasing use of DOACs in Australia and New Zealand in patients with obesity given the ease of administration and lack of monitoring required. Despite the recommendation to perform DOAC levels in this group of patients, interpretation of levels is difficult due to a lack of well validated therapeutic ranges with clinical correlation. Further data regarding the clinical utility of DOAC levels, appropriate dosing strategy for enoxaparin, and clinical outcomes in this population is required. Our registry provides data regarding drug levels in this population, prescribing characteristics and clinical outcome data.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

